It is often the case that good teachers just “intuitively” know how to teach. Whilst that may be true, there is now a greater need to understand the various processes that underpin both the ways in which a curriculum is delivered, and the way in which the students engage with learning; teaching excellence is increasingly in the spotlight, with various metrics being proposed at institution, discipline and school level.
Whilst many of the ways in which excellence is measured will depend upon graduate performance and success, there is also a growing interest in demonstrating fitness to practice and measuring levels of student satisfaction, stress and support. As such, curricula need to be designed to meet the changing needs of our new graduates, providing new, challenging and robust learning opportunities, and be communicated clearly and effectively to both staff and students.
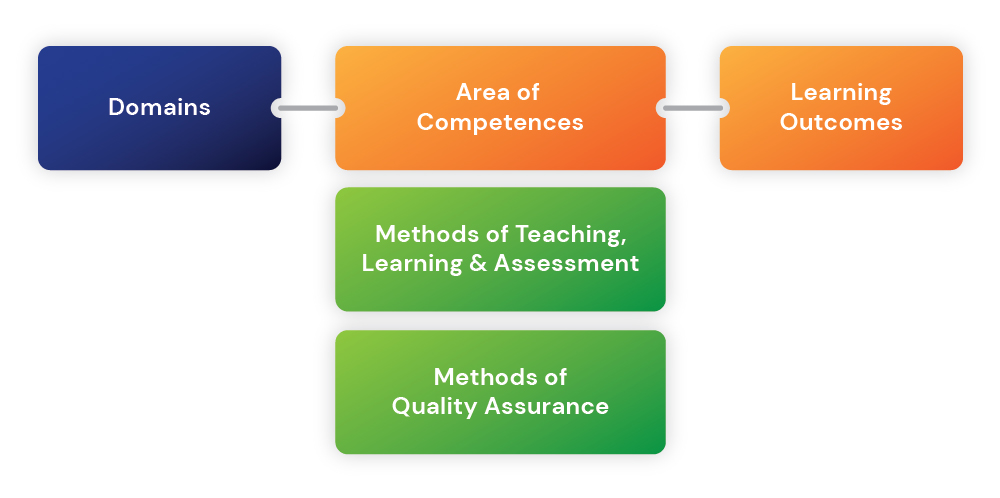
With these developments in mind, ADEE has published a new profile of undergraduate dental education in Europe for use by dental educators and other stakeholders in the form of a Framework—‘The Graduating European Dentist’. After wide consultation, the process has injected a fresh new approach that reflects best academic practice for European Dental Education. The Framework, displayed in Figure 1, comprises 4 Domains covering topics referred to as Areas of Competence. These are accompanied by a series of associated “Learning Outcomes”.
The 4 Domains comprise; Professionalism; Safe and Effective Clinical Practice; Patient‐Centred Care and finally Dentistry in Society
The aim of this secton is to draw together robust and contemporaneous methods of teaching, learning and assessment that help to overcome some of the more traditional barriers within dental undergraduate programmes. The methods have been chosen to map specifically to the 4 new Domains, above, and should be considered in parallel with the benchmarking process that educators and institutions employ locally. The methods of teaching and learning are not intended to overshadow wider strategic approaches (for example, the use of problem‐based learning and other curricular approaches) but instead, to provide some further guidance and inspiration for enthusiastic educators and interested institutions.
The document is by no means prescriptive, given the tremendous volume of original and reviewed literature that already exists describing general and medical approaches to teaching, learning and assessment (Williams et al. 2015, Huggett & Jeffries 2014, Harden et al. 2017) nor is there any attempt to explore issues around examiner training, calibration and bias. However, times are changing in terms of how we engage with educators and students—with a growing emphasis on professionalism and fitness to practice. To achieve this, students must be effectively engaged with a robust and comprehensively mapped curriculum. Assessment should be clearly signposted and mapped to objective rubrics, allowing both educators and students to demonstrate clinical competence. The final outcome should be the production of at least a “safe beginner,” who has the ability to provide effective patient‐centred care autonomously, and, on occasion, with continued guidance.
Methods of Teaching and Learning in Dental Undergraduate Education
The methods below are considered to be especially relevant to Domains I, II and IV.
A significant component of Domain II will relate to teaching and learning within a simulation environment, ensuring that students are safe to treat patients. The Association for Simulated Practice in Healthcare (ASPiH 2017) has consulted widely across different health care professions in this regard, and several of its recommendations are particularly relevant here:
- Faculty should ensure that a safe learning environment is maintained for learners and encourage self‐reflection on learning
- Faculty have a responsibility for patient safety and to raise concerns regarding learner performance
- Faculty are competent in the process of debriefing
- Simulation‐based education programmes are developed in alignment with curriculum mapping or learning needs analysis undertaken in clinical practice
- The patient perspective is considered and demonstrated within educational planning
Productive failure
This method of teaching provides an opportunity for students to devise their own solutions before they are given further direct instruction (Kapur 2008). It is recognised that whilst students often find this uncomfortable at first, the process often results in a deeper understanding of the problem. The student is said to be learning within a zone of “proximal development” (Vygotsky 1978), and the learning process should be clearly outlined to the students beforehand. This teaching method requires teachers to have a strong presence and have a deep understanding of the subject material and how the students learn; nonetheless, it can be incredibly rewarding. This form of teaching already exists within the dental clinical skills environment, in terms of both simulation and direct patient care. For example, when students are managing simulated caries or accessing/preparing teeth in the clinical skills simulation laboratory, or carrying out non‐invasive clinical procedures on patients, such as during complete denture construction. Teachers must avoid the temptation to demonstrate the solution, instead allowing the student to work themselves towards the intended clear endpoint with no direct tuition. Clinical skills teaching notes underpinned by this process of productive failure can be found online (Field 2015). Closely linked to the concept of productive failure is that of Bricolage or “tinkering.” This is especially useful whilst working with impression materials in the clinic, where it is important for students to understand how materials behave in their own hands, and how they may improvise to reach a clinically acceptable alternative solution. Whilst some students will report that knowing how to manipulate equipment/materials is “common sense,” for others there needs to be a degree of purposeful play and innovation, which can help to underpin fundamental concepts and approaches (Scanlon et al. 2014).
Threshold concepts
It is important for educators to be able to identify topics within the curriculum that might be considered as “threshold concepts.” These are concepts that normally require students to develop a qualitatively different view of the subject, “opening up a previously inaccessible way of thinking about something” (Meyer & Land 2003). A number of clinically relevant topics have been identified as threshold concepts, such as reflective practice (Joyce 2012), shared care (Wearn et al. 2017), and empathy (Ryan 2012), offering undergraduate clinicians important new perspectives. Identifying these important concepts can help educators to design curricula effectively, with tasks that engage students in thinking with, rather than about, a concept—ensuring that teachers understand the barriers and enablers to student uptake and correctly identify and support students struggling to move forwards from the “liminal phase” of old and emerging understandings (Neve et al. 2016). These topics should be introduced from an early stage and developed and reinforced throughout the clinical programme.
Teachback
This method is used widely within health education. In principle, learners need to be able to openly explain what they have learned in a way that is understandable. Encouraging “teachback” to colleagues/peers forces the learner to reframe what they know into accessible information. It provides a clear demonstration of shared understanding. This is very important within a clinical environment for communicating with patients, colleagues and the wider team. Teachers must be careful to select and supervise the activity carefully; otherwise, misconceptions can result in the different participants learning something incorrectly. Clinical examples of this are common; it should be embedded within the process and dialogue of peer review (most notably and accessibly within a clinical simulation environment). It should also form a significant part of a student's interaction with their patient (for example, when obtaining consent) and the wider dental team.
Tacit learning
It is not always possible for a teacher to explain how something is carried out, even if they themselves have mastered the skill. Nonetheless, careful observations and reflection can reveal a whole new experience for the learner—an untapped unspoken dialogue between student and teacher, which can map across a multitude of practical, behavioural, organisational and leadership domains (Fugill 2011). It is therefore important, wherever possible, to allow students the opportunity to observe clinical dentistry being practised by qualified, experienced and competent individuals.
Critical reflection
The process of critical reflection should be embedded throughout the undergraduate curriculum. At an early stage, students can be introduced to exercises that provide a framework for such reflection—for example through the recording of events, peer review or shadowing senior peers or tutors. As the concept of reflection is developed, an opportunity to reflect critically, emerges. Students can be shown the value of using personal reflections to create meaningful action plans and to track progress—and as a means of rationalising and selectively sharing the events that they experience whilst within the clinical environment. Grading matrices have been developed to help students and faculty overcome the threshold concept of critical reflection, and these have proven to be useful at both undergraduate and postgraduate levels (Field & Vernazza 2013). Reflection forms a valuable component of a student's (and in future a graduate Dentist's) comprehensive portfolio. The latter, including reflection critique, can provide a valuable learning tool for the Dentist's future clinical and professional practice. The philosophy of lifelong learning, including reflection on practice, commences during undergraduate training and remains embedded through the acquisition of quality CPD as a dentist remains up‐to‐date throughout their professional career.
Situated learning and role play
Within dentistry, the real‐time clinical environment and episodes of live patient care mean that clinical teachers are uniquely placed to role model for their students (Kenny et al. 2003, Oandsan & Reeves 2005). Clinical teachers can step in and out of patient care when they see fit, tailoring the learning episode to each student's needs. With such a small and closely dependent clinical team, it is also possible for students themselves to assume various roles. It is common for dental students to work in pairs, at least in the early clinical stages. In this situation, the clinical teacher must be observant and manage clinical pairings carefully. Desiree et al. (2016), talks about a careful balance of humour, managing interprofessional tension, debating styles and carefully selected learning activities, which can foster a concept of collaborative working. Ultimately, role modelling by fellow students or clinical teachers has been shown to impact on the ability of students to appreciate the importance of patient‐centred care (Wilcox et al. 2017).
Exchange programmes
Whilst there is little evidence evaluating behavioural change at the level of patient outcomes, much is made of cultural exchange programmes (such as ERASMUS) in relation to professional development, team working and communication (Scholes & Moore 2000). Abu Langhod (1994), argues that students experience minority status (when immersing themselves within a new cultural environment) and make connections that transcend stereotypical clustering. This, in turn, opens up new forms of understanding. Healthcare students that have experienced cultural exchanges report impacts at professional, educational and personal levels. They report a greater understanding about multidisciplinary teamwork, greater confidence to use research and rationale to support their actions, reflective insight into the way they could relate to patients and colleagues and enhanced understanding about non‐verbal communication (Scholes & Moore 2000, Lee 2004).
Blockchain learning
Blockchain learning is a very new concept within education but could lend itself well to professional development that requires a degree of longitudinal accountability (Sharples & Dominigue 2016). Traditionally, student records are held centrally and often fail to migrate with the student once they leave an institution or organisation. Blockchains of data are stored by individuals within a community, across many computers. They form a permanent record of someone's activity and cannot be altered or undone. It can be used to store qualifications, clinical activities, professional development activity or research/collaborative activities. It is intended to be linked to a currency of intellectual reputation and helps (within a profession) to embed a sense of accountability (blockchain.open.ac.uk). Blockchain learning is controversial, not least because it does raise some concerns about the trading of educational/professional reputations—but the concept of a comprehensive, unmodifiable record of clinical activity and competence, that is easily transported wherever an individual may work, is something that is already being embedded within some portfolio systems. This could strengthen the philosophy of a reflective portfolio of achievement providing the cornerstone and initial building blocks for lifelong learning.
The methods below are considered to be especially relevant to Domains I, III and IV (Professionalism, Patient‐Centred Care and Dentistry in Society).
A significant component of Domain III will relate to teaching and learning within the clinical environment, ensuring that students are able to provide care that is respectful of and responsive to individual patient preferences, needs and values. As such, several of the following methods make use of social learning environments and processes that encourage dialogue and reflective practice. It is also important for students to be able to observe the process of information gathering, diagnosis and treatment planning, by qualified dentists who are working within a real clinical environment. These observations will provide an opportunity for the tacit learning of a whole range of clinical, professional, time management and leadership skills. These, in turn, should support patient‐centred, professional oral healthcare delivery to patients.
Social media
The increasing prevalence of online social networks, within higher education, indicates the value that learners place on learning less formally, remotely and independently. Aside from providing a framework and a platform for accessible discussion, social media sites can also facilitate the reflective process—allowing users, in this case dental trainees/students, to defend their positions and “amend ideas in the face of criticism” (Sharples 2016). That said, there is a definite need for sites to be moderated appropriately, still offering appropriate learning opportunities, but provided in a more informal way. Given the “faceless” existence of online groups, the moderator or facilitator must be able to engage and enthuse students to keep them interested. In this sense, implementing and moderating the use of social media is relatively resource intensive. Within dentistry, it is common and popular for case scenarios and treatment planning to be discussed, along with photographs/images, online. This can happen within an internal organisational network, such as Blackboard (Blackboard Inc.) or Yammer (Microsoft), or closed social media groups such as Facebook. It is imperative that online discussion fora are closed from the public, secure, and that appropriate and explicit consent has been obtained before sharing patient‐sensitive information.
Threshold concepts and personal enquiry learning
Threshold concepts were introduced more formally in Domain II: they require students to develop a qualitatively different view of the subject. They are particularly important within this Domain III, where students are required to engage with a longitudinal application of basic science and fundamental knowledge that develops over time. We recommend that dental curricula account for a degree of vertical integration within a programme—allowing a longitudinal thread that links science with clinical decision‐making and treatment on a repetitive basis. This framework can be populated with learners from different academic stages concurrently, to make use of collaborative enquiry and active investigation—this is known more formally as “Personal inquiry learning” (Sharples 2012). By providing real clinical cases and examples for students across all undergraduate stages, students are motivated and engaged because they genuinely want to know the answer; they see direct value in engaging with the exercises, and as a result, are more likely to discuss and reflect on their findings with peers and tutors—even with subjects that are normally rather inaccessible and “dry” in isolation. In a true personal enquiry approach, student groups should be mediated at a distance, allowing the students to decide what and how they investigate and, ultimately, report their activities. For this to be successful, the students need to be provided with an “inquiry toolkit” (Scanlon 2011), and there needs to be a robust and respected method of information feedback/delivery by the students. Within dentistry, a regularly scheduled “case discussion forum” or “seminar” often works very well.
Storytelling
Linked to personal enquiry learning, and group case discussions, “storytelling” places emphasis on creating a narrative of student memories and experiences. It is in essence a story of the patient's journey through oral health care and the factors that have influence the outcomes. In contrast to critical reflection (which has a much more formal endpoint), “storytelling” should be encouraged from the very early stages of the curriculum. It is more formally known as “narrative pedagogy” whereby students and teachers share experiences collaboratively; problems and potential solutions are shared and explored through discussion and it is understood that there is no definite answer or endpoint (Ironside 2003). The need to create more of a balance between objectivity and subjectivity within the dental curriculum is already recognised (Smyth Zahra 2017). This approach can help students to be more tolerant of ambiguity. Over time, the concept of narrative pedagogy can be built upon, until eventually the students are familiar with the process of critical reflection. It is common for this transition to take place as students enter the clinical environment and begin to treat patients for the first time.
Fishbowl learning
Small‐group teaching can take many forms and is incredibly useful for developing skills in listening, questioning and responding (Edmunds & Brown 2010). There are inherent risks to forming small groups, most notably that participation is low, and teachers tend to dominate the dialogue. However, Fishbowl learning describes a strategy by which students are able to practise being both contributors and listeners within a discussion, whilst teachers assume a more facilitatory role. A circle of inwardly facing chairs forms the “fishbowl,” within which an active discussion occurs—questions are asked, and information, experience and opinions are shared. On outer circle of chairs requires students to practise being active listeners, paying close attention to the ideas that are presented, and the way in which they were uncovered. The outer circle participants should be reflective in nature, and students should be asked to swap between inner and outer circles at least once during each session. From a patient perspective, the outer circle can be particularly useful in creating opportunities for students to identify frames of reference and various forms of bias within a conversation.
Methods of Assessment in Dental Undergraduate Education
The methods of assessment below are considered to be especially relevant to Domains I, II and IV and apply to both the pre‐clinical and the clinical environments (Table 2 see published documents). More detailed information on the implementation and the concept of standard setting can be found elsewhere (Williams et al. 2015).
OSCE
The Objectively Structured Clinical Examination is a now very commonplace within the dental curriculum and is a useful way of consistently testing a range of practical clinical skills on a whole cohort of students. The OSCE examination is likely to be the most appropriate summative assessment to identify students that may be at risk of poor performance within a clinical environment (Terry et al. 2017). Typically between 8 and 20 “stations” are set, and students rotate through each station for a predetermined amount of time. Performances are graded against a set of “objective” criteria, and this type of test has utility across a wide range of skills such as:
- Communication and information gathering/transfer—taking histories, consent, communicating with the team, dealing with poor performance, whistleblowing
- Clinical skills—operative skills, surgery/clinic management, cross‐infection procedures, note taking
- Quality assurance and diagnostic testing—checking the quality of work, assessing records and formulating judgements leading to diagnoses
Clinical grading and feedback
Here, the students are offered feedback and grading after every patient contact. Whilst this type of feedback is demanding of staff time, it critically underpins the learning and reflective process whilst within the clinical environment. Clinical feedback can be offered both within the clinical skills simulation laboratory and the patient clinic. It is common for feedback and grading to be segregated into domains that facilitate discussion—often focussing on treatment quality, subject knowledge and aspects of professionalism.
Reflective diaries and portfolios
Based on the clinical grading and feedback that students receive, a portfolio system is recommended for recording the quantitative aspects of student activity and performance. This can be used to monitor student progress and compare activity to the wider cohort. Students should be encouraged to formulate reflective accounts, or “logs” of significant events. Such events should not be restricted solely to straightforward or complex procedures with a positive outcome. It is equally important to reflect on events which did not proceed as planned and the student is able to demonstrate reflection on “what could have been done better.” In time, this reflective analysis, by a student (and graduate Dentist), can provide the basis for a positive impact on future clinical and professional practice. All this information can be stored as part of an online portfolio system, or somewhere else personal to the student, with the option to share elements of reflection with others as the student sees fit. It is important that only the student can obtain access to the reflective component of this process and that records are stored securely; they should not contain patient‐identifiable data or other sensitive data.
Longitudinal observation
When clinical activity is recorded over a longer period, for example a term/semester, it can provide evidence about potential significant patterns of student activity. The main concern here is invariably related to underperformance, and the longitudinal data can be used to support students, direct resource and to objectively monitor performance in line with an improvement/action plan or performance review process.
Feedback from patients and other members of the dental team
Workplace‐based feedback is extremely valuable for both students and the educational institution. Whilst verbal feedback should be encouraged, written feedback provides a more permanent and accessible record of activity. Feedback can be collected overtly by the student from patients or colleagues, or anonymously, using standardised feedback forms. The forms can ask questions relating to a number of domains, such as clinical care, relationships with colleagues and professionalism. Students should also be in the habit of engaging with peer review at all stages.
Clinical competencies
Sometimes known on workplace‐based assessments (WPBAs) or clinical exercises, these competency‐based assessments can be used to critique examination, diagnosis, communication and operative skills. They can be used formatively, or students may be required to complete a certain number, or at a certain level, to progress. It is advised, within the pre‐clinical environment, that student clinical competence is assessed prior to the treatment of patients, as a means of safeguarding patient care—a “gatekeeper” for access to future treatment of patients.
Adaptive assessment
Within the pre‐clinical skills environment, adaptive assessment of operative skills can be a useful strategy to save resources and increase efficiency without decreasing validity (Muijtjens et al. 2000). This strategy has been used successfully to allow students showing clear competence in a range of clinical skills across the term/semester, to exempt themselves from the end of term examination; this directs valuable resources to students that are in need of closer support as they approach the examination. It is important that this approach is not used in isolation but is triangulated with other performance data (Schuwirth et al. 2002).
The methods of assessment below are considered to be especially relevant to Domains I, III and IV and apply to both the pre‐clinical and clinical environments.
More detailed information on the implementation and the concept of standard setting can be found elsewhere (Williams et al. 2015):
Written examinations
Most useful for assessing knowledge and the application of knowledge, the multiple choice (MCQ), extended matching item (EMI) and short answer question (SAQ) formats provide a reasonable amount of utility. MCQs are a way of asking students to select the correct (or most appropriate) answer from a list of options. They are an objective and efficient way of administering a test (Williams 2015). As students’ progress through their studies, it is appropriate to begin to implement tests/assessments which focus on the ability to evaluate information. Following an introductory vignette, the EMI requires students to select multiple answers from a long list of viable options. Both the EMI and SAQ are particularly suited to clinical scenarios—the SAQ requires students to formulate their own answers to a series of short questions based on a vignette. They are resource intensive in terms of writing, standard setting and marking but have been shown in dentistry to alter student learning behaviour and academic achievement (Pinckard 2012). More information on written test questions for clinical sciences is published elsewhere (Case & Swanson 2002). We have made little mention of essay questions, as reliability is low, marking is labour intensive, there is a high risk of examiner bias, and there is low validity in testing higher order cognition (Hift 2014).
Oral examinations
Whilst reliability is low, and the risk of examiner bias is high, oral examinations have utility in authenticating a student's ownership of a case (Williams 2015). The format involves the student being questioned by one or more examiners in relation to a pre‐defined context (usually a seen/unseen patient). Typically, oral examinations are reserved until the latter parts of a clinical course, when the student is expected to be able to understand and rationalise the treatment that should be/has been provided for a patient (Davis 2005).
Spotter tests
Increasingly developed as online tests, the spotter test is an opportunity for clinical students to display a working knowledge relating to the visual presentation of a patient, or their condition. A spotter test may function in much the same was as an OSCE (objectively structured clinical examination, see Domain II), and actually the questions may be served better as part of an MCQ or SAQ test, with improved reliability (Williams 2015).
Workplace based assessments
Building on the clinical competency tests discussed in Domain II, WPBAs are used to test practical competence within the clinical environment. Mini Clinical Examination (mini‐CEX) tests involve the student carrying out investigations with a patient and reaching a diagnosis. They can be used to assess history taking, physical examinations, diagnosis, decision‐making, communication and time management (Williams 2015). DOPS (Directly Observed Procedural Skills) are designed to assess clinical practical skills, resulting in a judgement of competent or not. Both the mini‐CEX and DOPS are usually recorded on a standard proforma across a number of domains, and the student is rated against a relevant standard (relating to the current stage, or in relation to a graduating dentist). It is recommended that these assessments are used formatively over time, in order for the student to build up a portfolio of their clinical competence, and their utility in dentistry is well documented (Norcini 2005, Durham 2007).
Case based discussions
The case‐based discussion (CBD) is another form of formative clinical assessment. Marked in a similar way to the mini‐CEX and DOPS, the CBD assessment takes the form of a detailed discussion between student and clinical teacher about the care that they are planning to or have provided for a patient. The clinician may discuss their clinician judgement and decision‐making, as well as their ability to record information accurately and contemporaneously. Adequate CBDs can be time‐consuming to carry out but offer a real feedback‐laden opportunity to the student with many dental trainees/students reporting an improvement in patient care following their administration (Kirton 2013).